Today I had the opportunity to listen to an energizing conversation between Dr. Yousuf Zafar, Chief Medical Officer of AccessHope, Jerrod Helms, Chief Revenue Officer of AccessHope, and Melinda Morimoto, HR Benefits Leader at Genentech. Together, they unpacked why cancer stands apart from all other health conditions employers manage — and made a compelling case for how an evidence-based approach drives both better clinical outcomes and meaningful budgetary impact. This is the work we do each day at AccessHope.
As AccessHope's Chief Marketing and Client Success Officer, I am not the clinician on the case or the actuary building the model — I am the person who has to look a benefits leader in the eye and say: this works, and here is what it means for the people on your plan. I also write this as someone who has been on the other side of a cancer diagnosis in my family.
This week would have been my dad's birthday. He has been gone 25 years — taken by a rare and aggressive stomach cancer when I was 19. Even with access to care and a family that asked every question we could think of, we reached the right answers too late.
Most of us carry someone. Cancer does not pause for anything, and none of us can afford to look away from it.
My dad was an engineer and a builder who believed the only worthy use of knowledge was to make something with it — something real, something that holds. This week, his birthday and this webinar arrived together, and I found myself thinking: this is exactly what he meant. This is how we build.
The Problem Nobody Is Talking About Plainly Enough
Cancer is now the top health cost driver for 58% of large employers. Cancer care among privately insured adults under 65 exceeds $156 billion annually, with employers absorbing nearly half. Costs are projected to reach $246 billion by 2030.
But here is the part that should keep everyone up at night — the benefits leader signing off on the spend, the patient trusting that the system has her back, the employer absorbing the cost: we are all paying enormously, with almost no visibility into whether the care is actually good. Screening adherence rates and enrollment numbers are not the answer to that question. Claims-validated, actuarially reviewed total cost of care reduction is.
Half of all cancer diagnoses occur in adults ages 20 to 64 — the core of the U.S. workforce. More than one in five employees is a cancer caregiver. Cancer is no longer a niche benefits issue. It is a strategic inflection point for cost, culture, and workforce resilience — and how an organization responds signals to its entire workforce whether they would be supported if they were next.
Why Cancer Is Unlike Any Other Condition in Your Benefits Portfolio
Cancer is uniquely difficult to manage because three compounding challenges have converged simultaneously — and most benefits strategies were designed before any of them existed at this scale.
A treatment knowledge gap. Cancer science is advancing unlike any other area of medicine. Lung cancer alone has evolved from a single disease into dozens of molecularly distinct subtypes, each with different biology, different treatment, and different evidence. There were over 50 new FDA indications in cancer last year — and oncologists are still learning to use drugs approved years ago as newer, more complex agents continue to appear. The volume of evidence a clinician must synthesize to make a guideline-based decision has grown 30 times over. No individual physician, however skilled, can hold all of it.
A diagnostic knowledge gap. Most new cancer drugs are approved alongside companion diagnostic tests. Yet genomic testing remains critically underused — only 35% of cancer patients currently receive proper genomic testing. Without the right diagnostic, precision medicine is impossible. You cannot target a mutation you have not identified.
Care inequities that follow every other fault line in our society. Early detection and screening are among the most powerful tools we have — getting diagnosed one stage earlier can triple survival odds and save tens of thousands of dollars. We need more of it, not less. But screening is the first step, not the last. Detecting cancer earlier only changes outcomes if the treatment decision that follows is correct. Right now, it often is not — and that is the gap that remains largely unmeasured and unaddressed. Only 60% of cancer treatment in the U.S. today is guideline-concordant. National Cancer Institute designated Comprehensive Cancer Centers produce meaningfully better outcomes, yet only 20% of cancer care is delivered there, and 80% of Americans live more than 60 miles from one. The result: differential care quality decided by where you live, who your oncologist is, and how well you can navigate a system that was not designed with everyone in mind.
An AccessHope study found that the highest odds of a treatment change recommendation occur in areas of greatest socioeconomic deprivation. The care gap is not random. Laying the blame solely on drug prices is an oversimplification — high costs and poor outcomes are driven by inaccurate decision-making, and that failure is not distributed equally. Getting underserved populations screened is necessary. It is not sufficient. The deepest inequity is not only in who gets diagnosed — it is in what happens in the exam room after diagnosis. The wrong treatment does not discriminate. But it lands hardest on the people with the fewest resources to recover from it.
60% of oncologists report burnout, and many are reducing hours or leaving the field entirely. The community oncologist goes room to room all day under crushing administrative burden — prior authorizations, documentation, insurance appeals — consuming the hours that used to go to learning. He is being asked to practice at the frontier of the most complex field in medicine, largely alone, with a full waiting room and no margin for error.
This is not a story about bad doctors. It is a story about an impossible system. And the consequences are visible in the claims data, if you know where to look.
What the Slide That Stopped Me Actually Shows
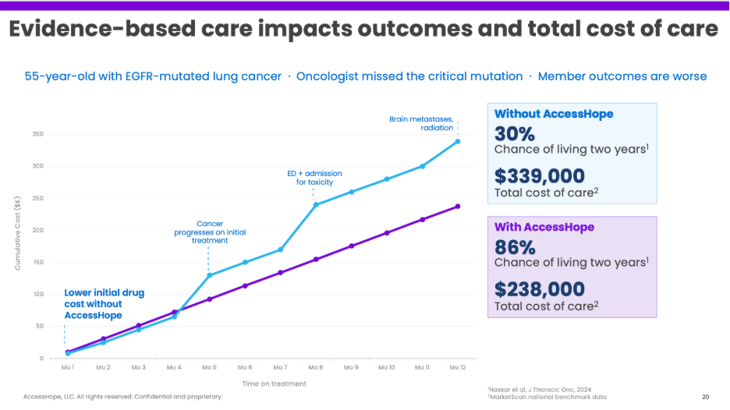
A patient with EGFR-mutated lung cancer. Her oncologist — a dedicated community physician — missed the critical mutation. She starts on the wrong drug. Cancer progresses. ED visit. Toxicity admission. Brain metastases. Radiation. More lines of therapy, each more expensive, each fighting a disease that never had the right opponent from the start.
-
Total cost of care at 12 months: $339,000
-
Chance of living two more years: 30%
Same patient, same oncologist, same hospital — but an evidence-based expert review happens before treatment starts. A subspecialist who has spent their entire career in exactly this cancer flags the mutation and recommends the right targeted therapy. The oncologist implements it. The patient never changes doctors, never travels, never fully knows what happened on her behalf before her first infusion.
-
Total cost of care: $238,000
-
Chance of living two more years: 86%
Nearly three times the likelihood of being alive. One hundred thousand dollars less. One decision, made earlier, made right. Where you live should not determine whether you live. But right now, for too many people, it does.
What Evidence-Based Care Actually Means — And How We Measure It
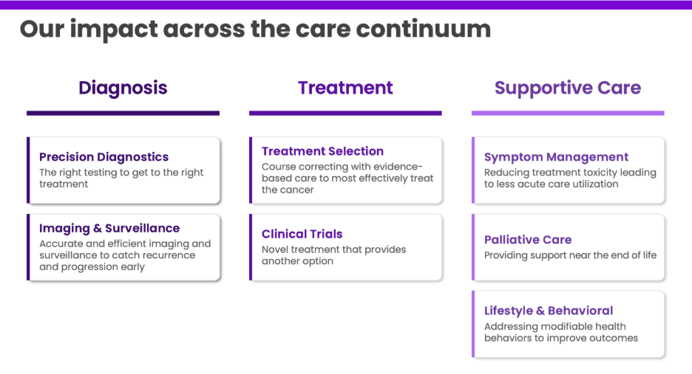
Evidence-based care is not a second opinion service, a navigation call center, or a virtual clinic. The community oncologist at the center of a patient's care is not the gap — the system around them is. What closes that gap is not a new clinical team built from scratch, but access to the subspecialty depth that already exists at the world's leading cancer institutions. The doctor who has spent twenty years exclusively in EGFR-mutated lung cancer is not a feature you can build. She is a relationship you must earn — with the institutions that train her, retain her, and concentrate her expertise. And she works alongside the local treating oncologist, not instead of them, applying the most current peer-reviewed clinical science to every decision across the full arc of a patient's journey — from diagnostic testing before treatment begins, to drug selection, to toxicity management, to clinical trial access, to end-of-life care. Catching what gets missed before it cascades.
People ask why we publish our methodology openly. The answer: the methodology is not the moat. Here is how the model works — and why the execution is what matters.
Step 1: Establish What Actually Drives Total Cost of Care
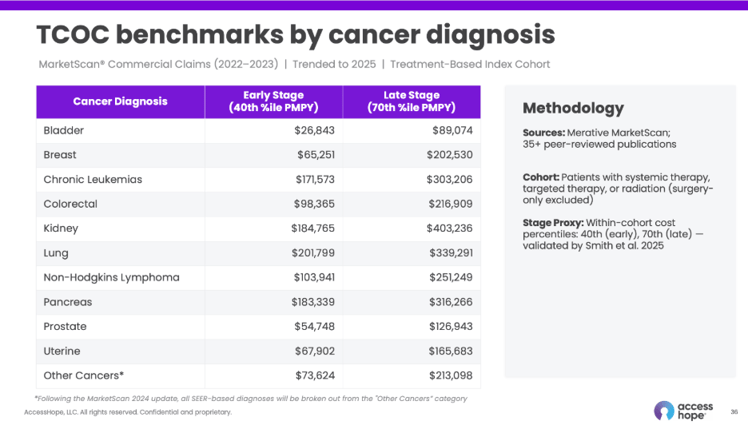
We partnered with an independent actuarial firm to determine what most influences total cost of care for a cancer patient. The answer: cancer type and stage — early or late. Comorbid conditions are present in the population and reflected in the benchmark — we simply do not take credit for savings related to them. For an actively treated cancer patient, the cancer is the primary clinical and financial driver, and the savings story should be grounded there.
Using the Merative MarketScan® Commercial Claims Database — the standard benchmark for commercial health economics research, covering millions of employer-sponsored enrollees — we built stage-stratified per-member-per-year (PMPY) benchmarks for each major cancer type, trended to 2025.
Step 2: Identify Which Interventions Reduce That Cost — and by How Much
We conducted a comprehensive review of the published literature — large-scale retrospective cohort studies, meta-analyses, and peer-reviewed health economics analyses from the New England Journal of Medicine, JAMA, Journal of Clinical Oncology, and JCO Oncology Practice, among others. This body of evidence consistently identified total cost of care reductions tied to specific, identifiable clinical interventions across the cancer care continuum, organized into seven Evidence-Based Care (EBC) categories:
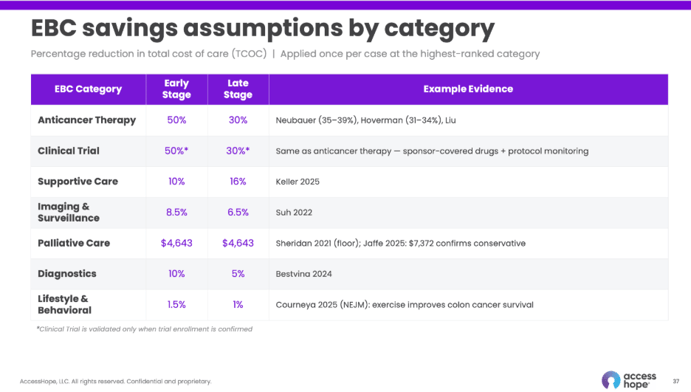
On average we generate two to three recommendations per case, many of which are adopted. But we take credit for only one total cost of care reduction per case — at the highest-ranked EBC category. No double-counting. A deliberately conservative architecture — because we would rather defend a number that holds than sell one that doesn't.
Anyone can report enrollment numbers. Anyone can show screening adherence improvement. The question a CFO should be asking is simpler and harder: show me the reduction in total cost of care, validated in actual claims, reviewed by an independent actuary. That is a truly short list of programs that can answer it.
Step 3: Apply This at Scale — This Is Where It Gets Hard to Replicate
The math is not the moat. The moat is the system needed to execute it:
-
Data infrastructure: We gather a unique dataset combining claims and medical records — with an 80%+ medical record fetch rate — to identify which patients would meaningfully benefit from expert review. Most programs cannot come close to that fetch rate, which means they are working from an incomplete picture of the patient.
-
Subspecialty expertise: We connect cases to world-class subspecialists at NCI-designated Comprehensive Cancer Centers — physicians who have spent their entire careers in specific cancer types. This produces recommendations precise and meaningful enough that treating oncologists adopt them in two out of three cases. The local treating oncologist remains the patient's doctor throughout — no disruption, no required travel.
-
Purpose-built AI: Our AI is trained on multiple datasets collected over years to do two things with precision: categorize recommendations by EBC type and detect in claims data when those recommendations have been adopted. That detection capability — confirming whether the intervention actually happened — is what makes the measurement credible and defensible. It is not a general-purpose model. It is purpose-built and deeply trained on oncology-specific patterns.
Without all three working together, the methodology is a spreadsheet. With them, it becomes a measurable, scalable system of care.
Step 4: Validate the Financial Impact in Actual Claims
We bring it together: the actuarially validated TCOC benchmark specific to the cancer type and stage, the literature-derived savings percentage for the highest-ranked EBC category, and the member's actual claims data for validation. The result is a total cost of care reduction that is specific, evidence-grounded, claims-validated, and actuarially reviewed.
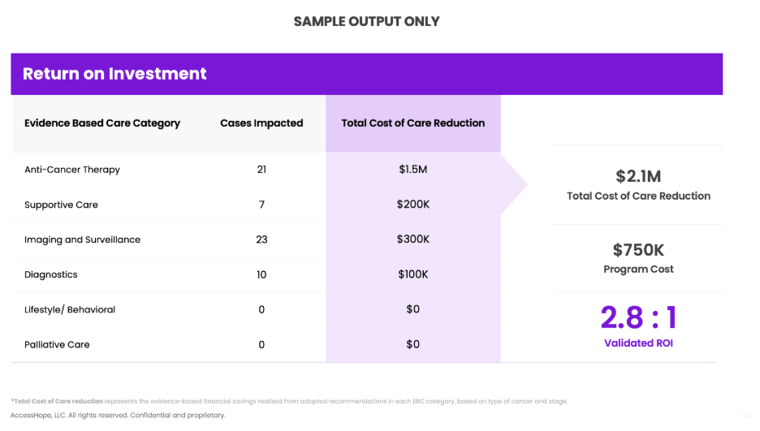
Measured in actual claims. Not modeled projections.
Melinda Morimoto and the team at Genentech built this into the foundation of their benefits program proactively — population-wide review across all cancer stages, not just the catastrophic late cases others wait for. In their population, roughly 90% of reviewed cases surface a meaningful clinical opportunity. Not a cost statistic — a measure of how many people were about to receive the wrong care and did not.
Step 5: Measure What Matters Most — Survival and Recurrence
The financial story is real. But it is a proxy for something more important.
AccessHope's outcomes model — connecting published clinical evidence on guideline adherence with our case identification rate and real-world oncologist adoption — estimates:
-
11.6% reduction in mortality risk For every 100 deaths that would otherwise occur, approximately 12 may be avoided (Modeled range: 9.7%–13.3%)
-
17.8% reduction in cancer recurrence risk For every 100 recurrences, approximately 18 may be prevented (Modeled range: 13.3%–21.0%)
Getting the initial treatment right has an outsized influence on whether cancer returns. And our own health equity research confirms that the impact is largest where the need is greatest — closing the evidence gap is, necessarily, a pathway to closing the equity gap.
The Questions Every Benefits Leader Should Be Asking
-
If an employee is diagnosed with cancer today, what does your benefits program do to ensure they are on the right treatment
-
How are you measuring treatment appropriateness — not just treatment cost — across your cancer population?
-
Can your cancer benefits vendor show you validated, claims-based evidence of financial and clinical impact?
The most vivid memory I have of my dad is the summer our whole family built a deck together. For every component — the concrete, the planks, the stain, the rails — he thought carefully about the job it needed to do. When we were done, we stood back and looked at something that would hold weight for decades. Not just making something — but making something that holds.
What AccessHope has built reflects that same approach — an intelligence layer grown from years of learning across claims, prior authorizations, medical records, and clinical data, deepened by sustained partnerships with the world's leading subspecialty oncologists, and validated in actual claims by independent actuaries. This kind of precision is not assembled — it is accumulated, case by case, study by study, year by year, until what you have made is something that holds.
The number that matters most to me is not the ROI. It is the 12 people out of 100 who don't become a statistic. The 18 families who don't get a second call with bad news. Someone gets more time — the kind that only feels ordinary until it is gone.
For those of us who carry someone, this is how we honor them — by building something that holds, long after they are gone. Happy birthday, Dad. And to everyone who pushed us forward: we are still building.
Watch the full EBN webinar featuring Dr. Yousuf Zafar, Chief Medical Officer of AccessHope, Jerrod Helms, Chief Revenue Officer of AccessHope, and Melinda Morimoto, Senior Benefits Director at Genentech.